Dysphagia
Dysphagia (swallowing difficulty) is a common problem encountered in the rehabilitation of stroke patients, head injured patients, and others with paralyzing neurological diseases. Dysphagic patients are especially likely to choke or suffer from aspiration (the entry of material into the airway below the true vocal folds), which may cause dire consequences including malnutrition and dehydration, degradation in psychosocial well-being, aspiration pneumonia, and even death.
Today's dysphagia management relies heavily on the videofluoroscopic swallowing study (VFSS). Even though VFSS is accepted as the gold standard, it requires expensive X-ray equipment as well as expertise from speech-language pathologists and radiologists. Hence, only a limited number of institutions can offer VFSS. As a result, VFSS has been associated with long waiting lists. Also, day-to-day monitoring of dysphagia is crucial due to the fact that severity of dysphagia can change over time. Certainly, VFSS is not suitable for such day-to-day monitoring.
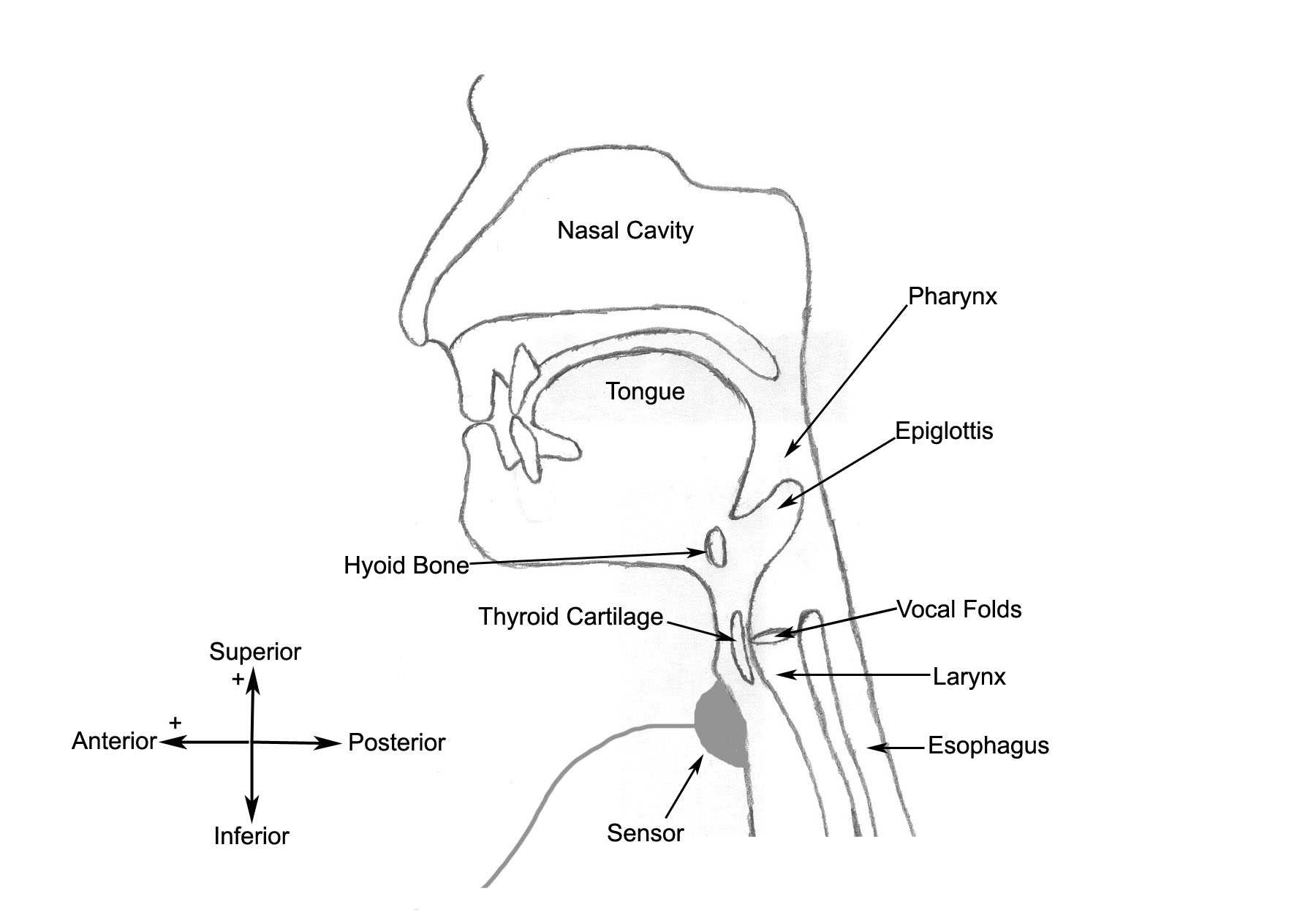
Cervical auscultation is a promising non-invasive tool for the assessment of swallowing disorders. It is being adopted by dysphagia clinicians as a component of clinical evaluation of swallowing. The cervical auscultation approach involves the examination of swallowing signals acquired via a stethoscope or other acoustic and/or vibration sensors during deglutition. One such sensing approach is swallowing accelerometry, which refers to an approach employing an accelerometer as a sensor during cervical auscultation. Swallowing accelerometry has been used to detect aspiration in several studies, which have described a shared pattern among healthy swallow signals, and verified that this pattern is either absent or delayed in dysphagic swallow signals. Although single axis accelerometers were traditionally used, our recent contributions showed that dual-axis accelerometers (as shown in figure below) yield more information and enhance analysis capabilities, since the motion of the hyolaryngeal structure during swallowing occurs in both anterior-posterior (A-P) and superior-inferior (S-I) directions.